The American Hospital Association estimates that workplace violence cost U.S. hospitals $18.27 billion in 2023. That number reflects lost productivity, staff turnover, legal exposure, and the operational drag of running a healthcare facility where nurses, physicians, and support staff face physical threats daily. A weapons detection system in a hospital is no longer a forward-thinking investment. It is a baseline expectation, and regulatory pressure is catching up.
California’s AB 2975 now requires hospitals to implement weapons detection screening policies for specified entryways, signaling where security requirements are heading nationwide. But choosing the right concealed weapons detection system is only part of the equation. Hospitals need a screening program that connects detection hardware to visitor management, real-time alerting, and coordinated response workflows across every entryway.
This page helps hospital security directors and health system leaders compare weapons detection technologies, understand what AB 2975 actually requires, and evaluate whether a platform approach fits their organization.
Why Hospitals Face a Different Weapons Detection Challenge
Hospitals are not courthouses, stadiums, or airports. Emergency departments cannot turn patients away. Visitors arrive around the clock. Contractors, vendors, and staff use different entryways with different access requirements. Restricting entry to a single controlled checkpoint is not operationally realistic for most healthcare environments.
That open-access reality creates a screening challenge unlike any other vertical. Bureau of Labor Statistics data shows healthcare and social assistance accounted for 41,960 of 57,610 nonfatal workplace violence DART cases in 2021 and 2022, representing 72.8% of the national total. Registered nurses faced a rate of 16.6 violent incidents per 10,000 full-time workers, compared to 4.3 across all private industry. Healthcare professionals face risks four to five times higher than private industry workers overall, according to The Joint Commission.
The consequences go beyond safety. Violence drives staffing shortages, accelerates turnover among staff members, increases legal liability, and erodes the trust patients and families place in a facility. A single screening device at one entry point does not address the complexity of these workflows. Hospitals need integrated screening programs that account for patients, visitors, contractors, and emergency arrivals, each entering differently and each presenting distinct risk profiles.
What California AB 2975 Requires for Hospital Weapons Screening
AB 2975 requires California hospitals to implement a weapons detection screening policy for specified entryways, using mechanisms, devices, or technology designed to identify instruments capable of inflicting death or serious bodily injury.
The law carves out handheld-wand-only screening as a limited exception for three specific cases: small and rural hospitals, entryways where spacing limitations mean another device would violate Title 24 accessibility or building standards, and hospitals exclusively providing extended hospital care. AB 2975 treats handheld-only screening as the exception rather than the default model. The law also requires response protocols for weapons detection events and alternative screening procedures for visitors who refuse screening. Meeting compliance expectations means documenting these protocols, not just installing equipment.
The Joint Commission’s broader prevention framework reinforces this direction. Detection alone is insufficient. Leadership oversight, written policies, incident reporting, data analysis, post-incident strategies, and staff training are all essential parts of the expected system. Even hospitals outside California should treat AB 2975 as a signal of where implementation standards are heading in the next budget cycle.
Why Handheld-Only Screening Falls Short in Most Hospitals
The operational math behind handheld-only screening does not scale. An older ASIS case example found that a single screening point required the equivalent of 4.3 full-time staff members during the week. While that figure is directional rather than current universal guidance, it illustrates the staffing intensity that manual wanding demands at every active entryway.
Throughput is the second constraint. Handheld wanding is inherently sequential. One person screens one visitor at a time, with no parallel processing and no AI backup. Operator fatigue and technique variation mean consistency degrades over a shift. There is no automated logging, no secondary screening documentation, and no way to monitor standardized protocols across operators.
Walkthrough and AI-assisted systems screen passively while the security team focuses on response. For hospitals evaluating technology options, the gap between handheld and walkthrough systems is about whether the screening program can sustain itself operationally across shifts, entryways, and facilities.
Comparing Weapons Detection Technologies for Hospitals
Hospitals should define their decision criteria before evaluating specific systems: throughput per hour, staffing intensity per screening point, false alarm profile, secondary screening workflow, accessibility (Title 24, ADA footprint), and integration with visitor management and response systems.
Here is how the major technology categories compare.
| Technology | Throughput | Staffing Burden | False Alarm Profile | Data Logging | Integration Capability |
|---|---|---|---|---|---|
| Handheld wands | Sequential, one at a time | Highest (4.3+ FTEs per point) | Operator-dependent | Manual only | None |
| Traditional walkthrough magnetometers | Moderate | Moderate | High (keys, phones, belt buckles) | Limited | Minimal |
| AI-assisted multi-sensor walkthrough | High (up to 3,600/hr reported) | Low (single operator) | Low (AI filters harmless items) | Automated, DHS-aligned | Full platform integration |
| Camera-based concealed-object detection | Passive, no walkthrough | Low | Emerging, still maturing | Varies | Limited |
| AI-assisted baggage X-ray | Continuous belt feed | Low (single operator with AI) | Low (material-type differentiation) | Automated with belt-stop | Platform integration |
Handheld wands carry the lowest upfront cost but the highest staffing burden. AB 2975 limits this approach to three exception categories for a reason. Traditional walkthrough magnetometers improve throughput but generate high false alarm rates from keys, phones, belt buckles, and medical devices. Every false alarm requires secondary screening time from your security team.
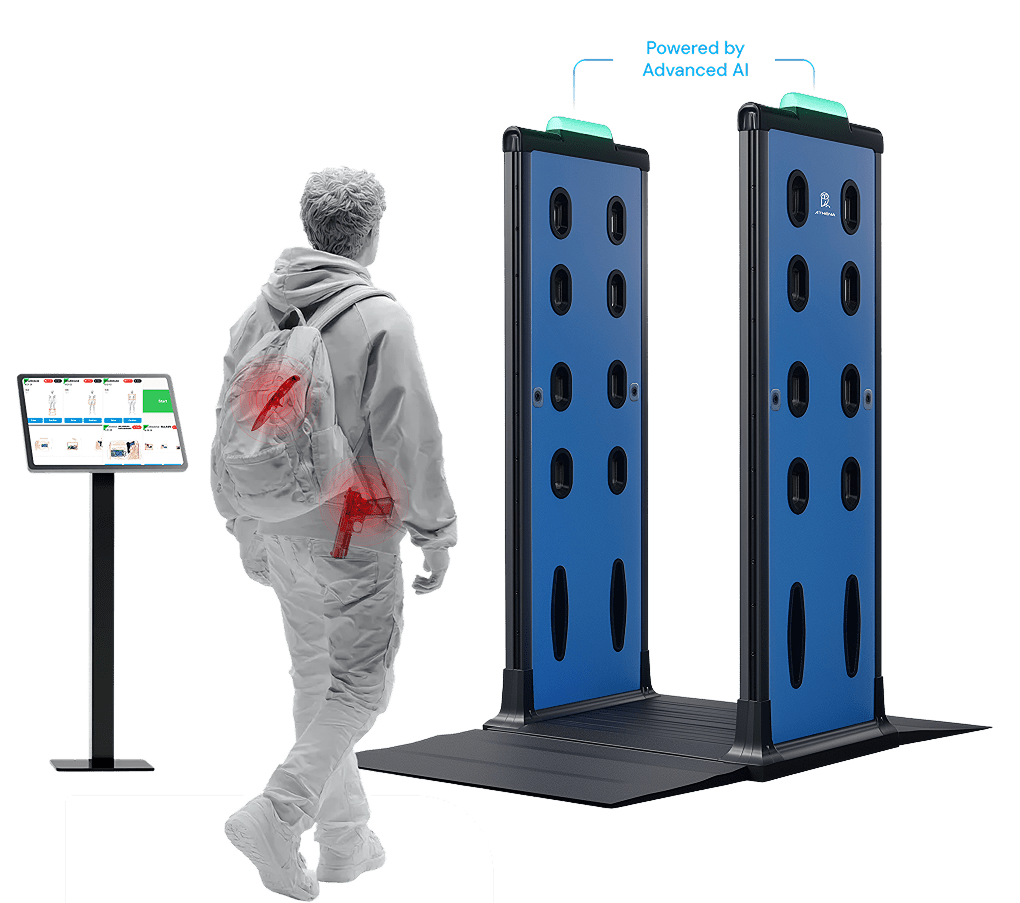
AI-assisted multi-sensor walkthrough systems represent the current standard for high-volume healthcare screening. These systems use low-frequency electromagnetic technology combined with computer vision to distinguish genuine threats from harmless items, reducing false positives and secondary screening burden. SSM Health’s deployment reported screening up to 3,600 people per hour at one facility. Athena’s Concealed Weapons Detection System falls into this category, pairing hardware from Apollo, CEIA Opengate, Garrett, or Metrasens Ultra with patented AI software that detects both ferrous and non-ferrous threats, including high-caliber assault weapons. The platform adds AI evasion detection to flag anyone who attempts to walk around the screening point, a capability Athena pioneered and patented.
Camera-based concealed-object detection offers passive screening without a physical walkthrough. This is an emerging category worth monitoring, but maturity and validation in healthcare settings are still developing.
AI-assisted baggage X-ray adds a secondary layer for bags and belongings. Athena’s AI Assisted X-Ray identifies firearms, knives, ammunition, explosives, and contraband in real time. Belt-stop technology holds items inside the machine while the operator reviews the alert, and the Workforce Multiplier feature lets a single operator manage both the walkthrough system and X-ray scanner from one console.
The volume flowing through hospital entryways demands technology that can keep pace. Cleveland Clinic confiscated 30,000 weapons in 2023. Hennepin County Medical Center identified 2,500 risk items in the first five months after implementing a screening system. Systems deployed in hospitals should also be third-party tested safe for pacemakers, implantable defibrillators, pregnant women, and other medical devices (look for EN 45502, ISO 14117, and ISO 14708 series compliance). Athena’s hardware meets these standards and uses dynamic non-contact detection with low-frequency electromagnetic technology.
How to Reduce False Positives and Screening Delays
Every false alarm costs your security team time, creates friction for visitors and patients, and erodes confidence in the screening program. Traditional walkthrough systems that alert on keys, phones, and belt buckles train operators to expect false positives. That means potential threats get less attention over time.
Athena’s AI-powered platform reduces false alarms by distinguishing between everyday items and genuine weapon signatures before an alert reaches the operator. The system enforces DHS best practices (14.2.2 Prohibited Items Log, 8.5 Secondary Screening Procedures) through built-in workflows so secondary screening follows a consistent, documented protocol rather than ad hoc judgment calls.
The platform’s AI oversight acts as an extra pair of eyes, monitoring operator presence and catching threats that might slip through due to fatigue, distraction, or multitasking during busy periods. If an operator steps away from their station, the system locks the connected iPad and notifies the appropriate team members. Fewer false positives means your security team can focus on real threats. Secondary screening becomes faster and more purposeful.
Why Detection Should Connect to Visitor Management and Response
A weapons detection system that operates independently from visitor management, alerting, and incident response creates gaps. Screening data in one system, visitor identity in another, and response coordination in a third means delays and information loss when seconds matter.
The Joint Commission’s prevention framework emphasizes that detection alone is insufficient. Policies, reporting, data analysis, post-incident strategies, and coordinated response must be connected. Athena’s platform is built around this principle. When a weapon is detected, the system simultaneously alerts security officers via tablet, mobile app, and AthenaVision AR glasses, logs the event for compliance, and triggers a response protocol. If the AI Assisted X-Ray detects a threat, it can automatically alert AR glasses and activate the Telepresence Security Officer with personalized visitor instructions at the entryway.
AB 2975 requires response protocols for weapons detection events. Those protocols are harder to enforce when detection and response live in separate systems.
Connecting screening results to Athena’s Visitor Management System adds the identity layer. Visitor check-in, badge printing, real-time watchlist screening, and access control create a complete record of who entered and what was found. For healthcare environments, the VMS integrates with Epic electronic health records and offers always-on offline capability so check-in, badge printing, and visitor logging continue during internet outages, server failures, or power disruptions. This integrated approach is the difference between a point product and a platform that helps protect everyone in your facility.
What Multi-Site Health Systems Need in a Weapons Detection Platform
A health system with 15 or 40 facilities may have different hardware at multiple locations, different staffing levels, and different entryway layouts. Security leadership still needs standardized screening protocols and centralized visibility across all of them.
Hardware agnosticism is the first requirement. Athena’s platform works across Apollo, CEIA Opengate, Garrett, and Metrasens Ultra systems, allowing protocol standardization without forcing equipment replacement at every site. Centralized cloud management through the Athena Control Center gives security leadership a single dashboard to monitor screening activity, compliance status, and incidents across all facilities.
The 72% industry-wide security staffing shortage makes it impossible to staff every entryway with full-time operators, so the technology must multiply existing staff rather than demand more headcount. Athena’s Workforce Multiplier lets one operator manage both weapons detection and X-ray screening from a single console. The Telepresence Security Officer allows one remote operator to secure up to four entryways simultaneously with life-size holographic interaction. DHS best practices are enforced uniformly through the platform, not reinvented site by site.
Multi-site deployments are already proving this model works in healthcare institutions. Duke Health runs 21 screening locations on a single Athena platform. Lamar Consolidated ISD deployed 24 Athena systems district-wide. Indiana Regional Medical Center integrated weapons detection with visitor management into one system, with their Security Manager noting it saved both time and money while making processes more standardized and efficient.
No threat detection system can guarantee 100% effectiveness. Detection solutions should be used as part of a comprehensive, multilayered security strategy.
Frequently Asked Questions About Hospital Weapons Detection
Do hospitals use weapons detection systems?
Yes, and adoption is accelerating across the country. Regulatory mandates like California’s AB 2975 and rising workplace violence are driving healthcare systems to install walkthrough and AI-assisted screening at emergency department and main entryways. The Joint Commission now includes weapons screening in its broader violence prevention framework for healthcare safety. Athena’s platform is deployed across major health systems including Duke Health and Memorial Hermann.
What does California AB 2975 require hospitals to do?
AB 2975 requires hospitals to adopt a weapons detection screening policy for specified entryways. Beyond hardware, the law mandates written response protocols for weapons detection events, alternative procedures for visitors who refuse screening, and compliance documentation connecting screening activity to facility safety programs. Athena’s platform automates compliance documentation through built-in DHS best practices workflows, including the Prohibited Items Log (DHS 14.2.2) and Secondary Screening Procedures (DHS 8.5).
Are traditional screening methods enough for hospital security?
For most hospitals, no. Handheld wands require one operator per visitor at a time, cannot log data automatically, and produce inconsistent results as operators fatigue over a shift. AB 2975 classifies handheld-only screening as an exception limited to specific facility types, not the standard approach for general acute care hospitals.
How do hospitals reduce false positives during weapons screening?
AI-powered systems filter harmless items from genuine weapon signatures before triggering an alert. Athena’s patented AI software distinguishes everyday items like keys and cell phones from concealed weapons, reducing the false alarm volume that desensitizes operators over time. Structured secondary screening protocols based on DHS best practices ensure that when alerts do occur, the response is consistent and documented rather than based on individual judgment.
Can weapons detection work in emergency departments without slowing patient flow?
Yes, when the system is designed for high throughput. Athena’s AI filtering reduces the secondary screening burden so patients move through faster. The system detects both ferrous and non-ferrous threats passively, without requiring manual wanding or sequential processing at each entry point. Facilities using AI-assisted walkthrough systems have reported screening up to 3,600 people per hour.
How should hospitals handle secondary screening after an alert?
Follow documented DHS best practices for secondary screening procedures. Trained operators should conduct secondary screening using a standardized protocol (DHS 8.5). Athena’s platform monitors secondary screening in real time, logs every interaction for compliance and incident review, and alerts supervisors if procedures are not followed. Consistent procedures protect both the facility and the screened individual.
How do weapons detection systems integrate with visitor management?
Through a shared platform that links detection data to visitor identity. Athena connects weapons screening directly to its Visitor Management System, so badge printing, watchlist screening, and access control work together. For healthcare environments, Epic integration links visitor records to patient information. Your facility maintains a complete record of who entered and what was found, with no gaps between systems.
What should multi-site health systems look for in a weapons detection platform?
Hardware flexibility, centralized cloud management, and standardized compliance enforcement. Athena’s platform works across Apollo, CEIA Opengate, Garrett, and Metrasens Ultra systems so each facility uses the hardware that fits its entryways. The Athena Control Center gives leadership a centralized dashboard with visibility across all locations without requiring site-by-site configuration or additional headcount.
Are weapons detection systems safe for patients with pacemakers and medical devices?
Athena’s compatible hardware is third-party lab tested to EN 45502, ISO 14117, and ISO 14708 series standards, confirming safety for cardiac pacemakers, implantable defibrillators, and other medical devices. The systems use low-frequency electromagnetic technology and dynamic non-contact detection that meets EMC electromagnetic radiation standards. They are safe for pregnant women, children, and electronic devices.
What happens when a visitor refuses weapons screening at a hospital?
AB 2975 requires hospitals to have alternative screening procedures in place. Facilities should document a written protocol for refusal scenarios that balances safety with patient access rights. Athena’s platform logs refusal events and routes notifications to the appropriate security team members. Response procedures should address de-escalation, notification, and documentation of the refusal for compliance records.
Learn More About Hospital Weapons Detection
We help hospitals connect weapons detection, visitor management, and response into a single platform built around DHS best practices. Book a Demo or call 833-928-4362 (1-833-9-ATHENA).